Back to Professional Projects
Sharp Healthcare, San Diego
Sharp Healthcare, San Diego
Patient Management Workflow & Clinical Deliverables
Sharp Healthcare, San Diego
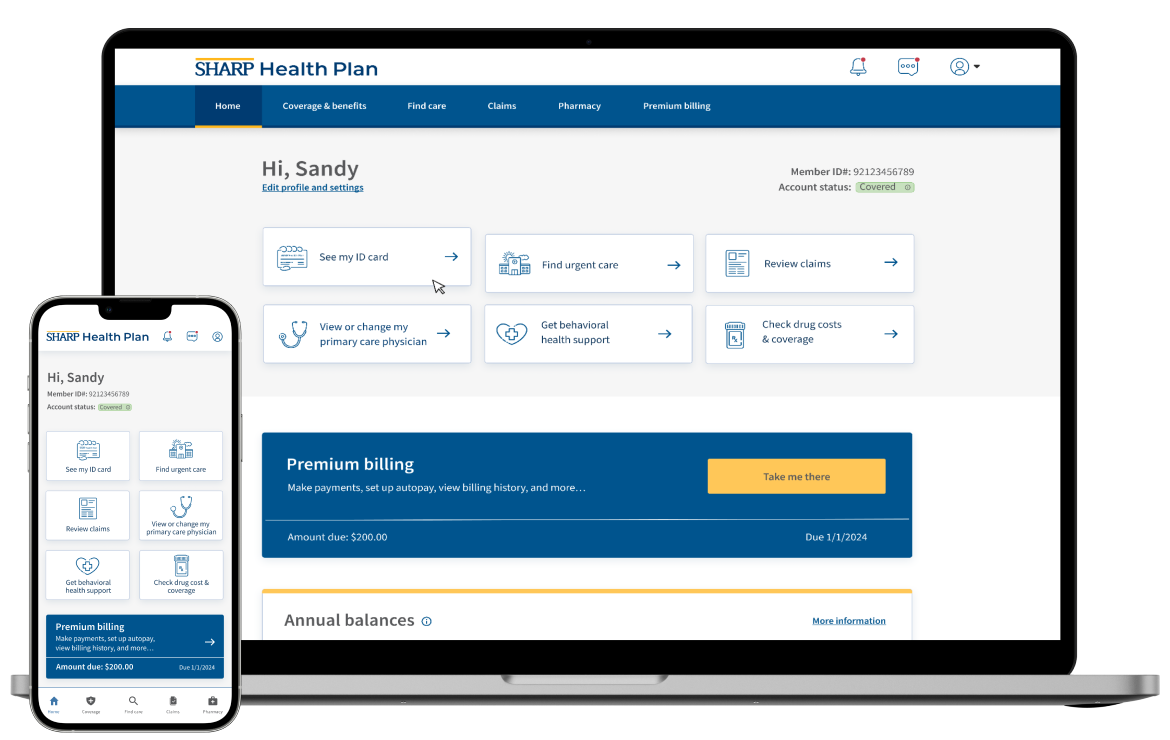
At Sharp Healthcare I work across clinical, operations, and reporting teams to improve how patients move from first contact to being seen. This project focused on untangling the patient management workflow, tightening expectations for key clinical deliverables, and giving leaders clearer, faster visibility into what is happening on the floor.
The work combines process mapping, requirements, UAT, and reporting into one view of the patient journey so teams can see where time is lost, agree on what “good” looks like, and measure whether changes are actually working.